

Last week, in very short order, eight members of the New York Yankees, all of whom were apparently “fully” vaccinated, tested positive for COVID-19, confusing and alarming many Americans — not to mention Yankee fans — who had assumed that vaccination would close the book on the pandemic, at least for the vaccinated. Michael Mina, however, was not confused or alarmed. A Harvard epidemiologist who has spent the pandemic advocating for the widespread use of home-pregnancy-style rapid antigen tests, Mina has become, over the past year, one of the most clear-eyed critics of the public-health establishment and the COVID messaging that has emerged from it.
It seems like you don’t think these are “breakthrough” infections and also that you’re not surprised to see them.
The Yankees are testing themselves frequently. When that happens, especially if you’re doing PCR tests, you’re going to find exposures and infections.
Even in people who’ve been vaccinated?
Yes. I’ve always said that it is very unlikely that these vaccines will create fully sterilizing immunity. Sterilizing immunity is the kind of immunity where, if you get exposed and the virus lands in your respiratory tract, it will be neutralized (or killed) immediately. It will not have a chance to replicate. On the other hand, you can have very highly protective vaccines that are not fully sterilizing — vaccines that prevent you from illness, especially severe illness, but may still allow the virus to grow.
And a PCR test would catch those kinds of infections?
This is a technology that can catch just ten molecules of virus. But this is a virus that when it is contagious, there are billions of molecules. So we have to be very careful about how we interpret PCR results. Just because the virus can grow a bit — and be detected on a PCR test — does not mean we are stuck in the woods as far as herd immunity goes. A vaccine that doesn’t create sterilizing immunity can still greatly limit virus growth, perhaps enough to massively limit transmission. This is likely the case with the mRNA vaccines at least, given the large reductions in cases among kids in hospitals as a result of the adults getting vaccinated. Clearly transmission declined significantly enough to elicit some level of herd effects on the kids.
But it probably won’t decline to zero.
As I have been saying since last summer, we should expect reinfections following infection or vaccination. This should not come as a surprise to anyone. The real question is do those reinfections matter — or more to the point — do the reinfections have negative consequences?
Do we not have to worry about infections of that size?
In my opinion, if they’re not infections that are causing disease, they should be viewed very differently from a breakthrough case, which is a term that should absolutely be reserved for a case that’s causing disease.
Why?
A breakthrough case is a case where the diseases is literally breaking through the type of protection we expect the vaccine to provide. And the clinical trials of the vaccines and their authorization hinged on whether they prevented disease in the vaccinated individual, not based on their ability to stop spread.
So a breakthrough case would be only when someone actually gets sick? Unfortunately the CDC has mixed this message up – at once calling these breakthrough cases and simultaneously suggesting that the cases don’t matter and not to get tested if vaccinated. This is very confusing for people.
How can we distinguish between an infection we don’t have to worry about and one that could cause sickness and be transmitted?
The simple answer is that we can look at viral loads. Now that the vaccines are being rolled out, the story is going to come out in a much more robust fashion. But it’s the same story that I’ve been telling this entire pandemic: Extraordinarily low viral loads should not, right off the bat, be considered infectious. Instead, we’ve taken the opposite approach: If you’re positive on a PCR test, you’re considered infectious, and you should isolate, no questions asked, no nuance of what that PCR result means.
But a lot of people aren’t actually infectious when they’re PCR positive — it’s just a little bit of virus replicating but not enough to necessarily transmit and certainly not enough to warrant a ten-day isolation anymore. You can test positive on a PCR machine for up to four or five weeks after you’ve stopped being infectious, which can be a period as short as just three days. Sussing this out is where antigen tests come in.
These are the rapid tests we’ve discussed before.
They will only really turn positive when you’re truly positive and infectious.
Another way to put it is that, when it comes to public-health testing, the PCR test is full of false positives. To be clear, they are real positives, biologically, meaning the primers are actually binding the correct viral RNA, there is actually SARS-CoV-2 there, but does it always necessarily mean you have to isolate? If you are no longer infectious and the PCR test is telling you you are positive and that is interpreted as needing to isolate, then I would call that a false positive from a public-health perspective.
What proportion of positive tests are we talking about?
Around 60 to 70 percent of the time that you’re PCR positive you are post-infectious. What that means is that the vast majority of people that we detected and isolated, we isolated in error — or rather, people isolated when they probably didn’t have to. They were already done with being infectious by the time they got a swab put into their nose. That’s not to say isolation never would’ve helped, just that the period when it would have been effective might’ve been 1 or 2 or even as many as 5 weeks earlier, when they were actually contagious.
For certain things, of course, PCR is the right clinical tool. Just like a forensics detective wants to use a particular tool to pick up shreds of hair or DNA at the crime scene — a PCR is good for that kind of approach, where you want to make sure you find the tiniest bit of virus to help reconstruct, in this case, why someone was feeling unwell. But you don’t need a PCR machine to actually see the equivalent of when a crime is currently being committed. You just need your eyes. That’s what antigen tests do, they tell you whether the infection is serious enough to merit isolation. If we had adopted that strategy, the whole notion of a ten-day isolation period or 14-day quarantine could have disappeared. We could have said, look, if you’re positive on PCR, then for the next week, use an antigen test or a rapid test daily at home, and once you hit two consecutive days of negativity, you can leave isolation. That would have led to so much greater compliance.
The same thing with quarantines. We could have actually done away with onerous and inefficient quarantine altogether. If we said, “Look, use a rapid test daily, and as long as you’re negative, go back out … All it takes is 30 seconds of effort in the morning each day. If you want to be really safe, do it twice a day, one in the morning and one after lunch.” That’s a whole lot better than staying in your house for 14 days. We could have put those pieces in place, but we had a medical establishment and a rigid public-health apparatus and a couple of regulatory agencies that were pretty much completely unwilling to look at the biology and the science and only willing to look at … Well, frankly, they weren’t looking at anything. They were just looking at dogma.
But the vaccines are now going to make this glaringly obvious because people are going to be testing positive, and the CDC is going to want to be able to say, you know, you’re still protected.
But you are protected, right, at least from real illness?
Yes. This is an infection, but it’s not not likely to lead to transmission or real sickness — it’s a low level infection. And I bet what we’ll see from the CDC is a little damage control.
What would that mean?
Trying to push for CT values to be reported, and not just positivity or negativity of a test. Or, to be able to deal with this, they may just take a blunt hammer to it and go so far as to just say “if you’ve been vaccinated you don’t need to test” which I think would be a major mistake. Better to use the right test with the right interpretation for the job then to just remove it altogether.
In other words treating infection as much more of a spectrum, when throughout the pandemic we’ve treated it much more as a binary matter.
Right. The way we’ve been using PCR thus far is the equivalent of saying that you either are completely immune to a disease, or you’re completely vulnerable. But we all know that you can get a little bit sick or you can get a lot sick, and that those are two really different things.
That had its own cost throughout the pandemic, of course, but it’s also meant we’ve sort of poorly educated the public about how to navigate the post-pandemic, as this episode with the Yankees shows.
That’s exactly right. Binarizing all of these results, and continuing to put everything in black and white — that has been immensely destructive. One of my core philosophies in public health is we absolutely need to bring the public along. You need to keep them up to speed. You need to keep them informed. If you don’t have the public buy-in for everything you’re doing, you will never defeat a pandemic.
Throughout this pandemic, we’ve generally considered the public to be the problem. But this is public health. The public isn’t the problem – that’s on the virus – instead, the public is the solution. As we are seeing with vaccines, the public is the solution and unless we want to vaccinate people based on some forceful military state requirements (which we do not and I hope never would) then we must see the public as the solution, always.
So we need to bring the public along. You need to keep them up to speed. You need to keep them informed. If you don’t have the public buy-in for everything you’re doing, you will never defeat a pandemic. What we’ve done instead, by assuming that the public was unable to deal with this kind of information and this kind of nuance, we have done immeasurable damage.
We’ve made the same mistake with herd immunity — treating it as some threshold before which there’s still great danger and after which there is none, rather than a gradual lessening of risk as more people gain immunity through infection or vaccination.
It’s crazy. Why we continue to treat everything as black and white from testing to disease to herd immunity is … I can’t really figure out why. Maybe it’s just a basic human thing, but I think it’s something our CDC and our FDA and our policymakers should’ve done a much better job educating about. The burden really falls on them.
Putting aside the CDC and the FDA—to the individual lay person, what is the threshold to be thinking about? In a PCR test, viral load is measured by CT value, which is a confusing inverse value — the higher numbers mean less virus. What is worrisome and what is not worrisome?
Unfortunately it’s a bit hard for the average person to understand, in part because the FDA and the CDC never pushed for standard curves to be used in laboratories, and so a CT value of 30 in one lab might be a CT value of 22 in another lab. And there’s almost a thousandfold difference between the two numbers. But if I were forced to give a single value, a value of 30 or above is generally where we start to see the viral culture really diminish to zero, and it’s the threshold where we see antigen tests go from positive to negative. So a CT value of 30 is a good metric to consider — if you’re below that, you should probably consider yourself infectious.
But below 30 is a massive range of about 1 million-fold. A 15 is about 1000 times more virus than a 25 and a CT of 5 is about a thousand times more virus than a 15, or a million times more than a 25. The scale is exponential. And the gradients really matter. Humans are really bad at understanding logarithmic scales or exponential growth, which is what these CT values measure. To put it in perspective, when people really are transmitting they’re at a million or a billion times higher viral load than when they have a CT value of 35. Treating them as equivalently “positive” — it’s like you give ten dollars to a homeless person and then describe both him and Jeff Bezos as “flush.”
It’s a pretty good argument against using logarithmic scales for almost anything, which is something I’ve thought a lot about before regarding earthquakes and the Richter scale. An earthquake that registers a six on the Richter scale isn’t a little bit bigger than one that registers a five — it’s ten times bigger! And an eight is a hundred times more intense — meaning a thousand times more intense than a five. I think very, very few people understand that, and I could never figure out why we talked about earthquakes in those terms anywhere but possibly in the most technical papers.
You’re absolutely right. And whether you’re looking at viral load over time at linear scale or logarithmic scale makes an enormous difference. Hang on, I’m going to text you something. Did you get it?
Yeah.
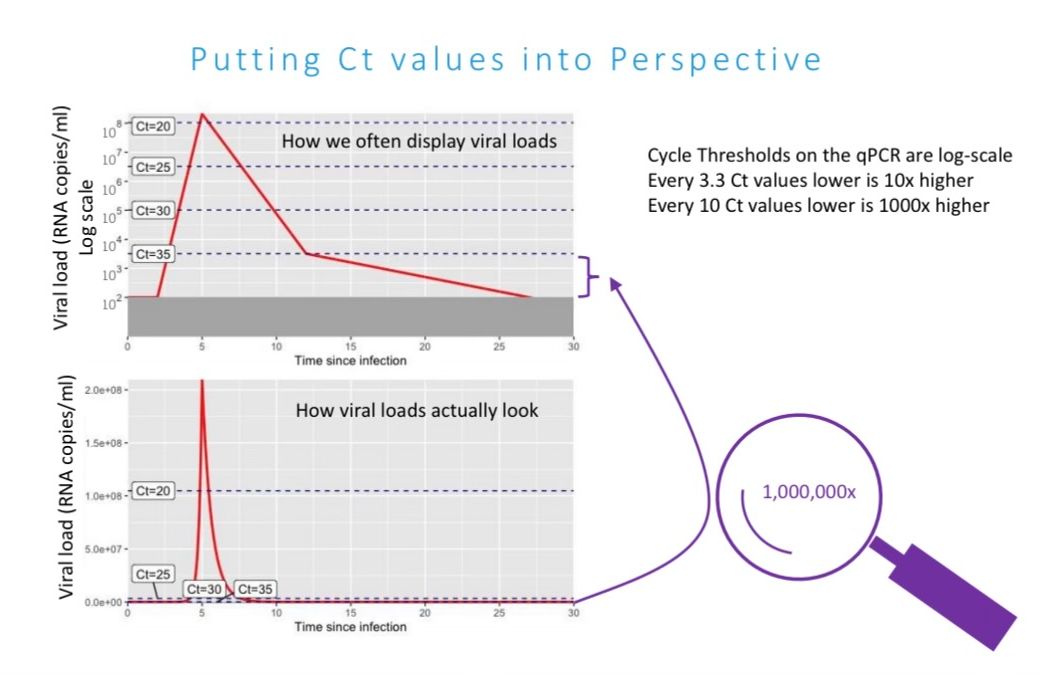
This is exactly what I’m talking about. These are identical curves. On one, you think you might be transmitting for 20 days. On the other, it’s clear that you’re actually only transmitting for four.
But the measurement is the same.
It’s astounding. Using these logarithmic scales for CT values and not immediately trying to convert back to a linear measure of viral load has been highly detrimental.
It’s the difference between using numbers that are close together to describe huge differences in viral load or using numbers that actually illustrate the difference.
Yeah. To one person you say, your viral load is a thousand, and to another, a trillion. I hope that people would be able to intuit that those are very, very different viral loads.
Does that mean you think that a lot of the cases throughout the pandemic maybe shouldn’t have been treated as true positives — by which I mean, infections actually likely to cause illness and transmission?
That’s correct. We should have been much more discerning about how we used and interpreted the PCR results. I published on the need to interpret the PCR Ct values in a paper at the very beginning of this pandemic and suggested that many if not most PCR positive people no longer need to be in isolation—we missed the boat on those people. Most people only made it in to get the PCR test or only eventually got the results after their period of transmission was good and done. In fact, when PCR tests were taking 10 days to return, then if you got a positive result then the understanding of that should have been: I’m done with my isolation window of time. Unfortunately I may have spread the virus already, but now I no longer need to isolate.
Unfortunately people have interepted these criticisms as assuming the PCR result is flatfly false and using it to acll this a “case-demic.” I hate when people say “casedemic” — this is not a “casedemic”! Each PCR positive person is a real positive, but we were just too slow and inefficient with our testing to make most if it worthwhile. Moving forward, we don’t want to find ourselves continuing to isolate people just because they are found to be PCR positives.
Of course it’s not a casedemic — we have hundreds of thousands of Americans dead. But it seems that one implication of what you’re saying is that perhaps many fewer people were actively transmitting disease than we counted along the way as positive cases.
Well, I think this requires a slightly different language to discuss, depending on what your purpose is. If I’m trying to monitor the spread of the virus, then the simple question is, has this person been infected? And in that sense all of the cases have been real cases, with the exception of a really very small percent of false positives. But if your question is how many people have shouldered the burden of this virus from a physical perspective, then that’s a really different number.
It seems somewhat related to the matter of superspreader dynamics, where a vast majority of cases are produced by a sliver of infections.
Yeah, I would say that’s exactly right. But what we see is the variation of viral load within a person is much, much greater than the variance of viral load across people. A paper came out recently that showed 90 percent of the viral particles in a population were held by just 2 percent of the people. Well, that’s true, but what really has to be taken into account is that those people change daily. Most people who get an infection, they’ll probably go through a period of time where they can contribute to that 2% of people holding 90% of the viral particles and be a superspreader, but that time period is so short. You might be infected for three or four or five weeks, but if you walk into a bar in a certain three day window, you might not just be a transmitter but a superspreader. But if you were to walk into that same bar, five days later, with same infection, you’re still PCR positive, but you might not transmit to anyone because your viral load will be a million or a billion times lower than it was just a few days earlier.
Which does emphasize the need for rapid testing — the faster the viral dynamics change the faster you need your diagnostic tools to work.
The only way you’re ever going to stop transmission is if you find people who are about to hit that really high viral load or are already in the middle of it and isolate those people, even for just three or four days until they pass peak infectiousness. If you’re not doing frequent testing, you’re very unlikely to just happen to stick a swab into somebody’s nose in the day or two before they hit those really peak numbers. Most of the rest of the time, if you get a positive reading you’re getting it when you are no longer infectious.
Which means, I guess, that using PCR testing to guide isolation or quarantine is a really crude approach, which is going to lead to many times more people being isolated for much longer than is necessary. It’s almost an argument against using PCR tests at all, and just using antigen tests instead.
The whole thing with needing to get a PCR test within three days of getting on a plane, for instance, that’s so incredibly dangerous compared to a rapid test, because you could be negative one day and then, two or three days later, you could be at your absolute peak viral titers — like trillions of viral titers. Whereas if you were to use an antigen test right before that event, even if the antigen tests a thousand times less sensitive, you would absolutely find the people who are transmitting, and would have almost no risk of somebody walking in who’s a super spreader. It’s a remarkable lack of insight into the viral load kinetics by our policymakers to push for three days earlier PCR testing instead of a rapid test immediately before.
So is there really nothing surprising or strange about the Yankees outbreak? I understand everything you’re saying about low-grade infections, but still… We’ve been told that vaccines are effective at reducing transmission by something like 70 or 80 percent — those are estimates, of course. They’ve got eight people who tested positive — how can that happen? Isn’t that a lot?
Yes. It’s certainly a lot. But I think they got the Johnson & Johnson vaccine, and although that vaccine is working, it performed more poorly overall than even a single dose of an mRNA vaccine. Is it stopping severe disease? For sure. But it’s my feeling, given how it performed relative to the other vaccines in terms of just stopping any symptomatic disease, I wouldn’t really expect it to actually do a particularly great job at preventing transmission or acquisition. Hopefully it will do a very good job at preventing people from dying and reduce transmission. But fully prevent it? I doubt it.
That’s why we have to disentangle severe disease from symptomatic disease from asymptomatic acquisition and PCR positivity. And those are very, very different pieces. Unfortunately, again, we’ve had no nuance in our overall discussion at the national level, and it has really conflated all of those. We’re using the same word for all of those different things, and and that’s a really bad idea because it leads to fear and concern and confusion.
How does this all relate to mutation and variants? As vaccination has been rolled out, there’s been growing public concern about the risk of new variants arising in the “reservoirs” of still-vulnerable people — either in the U.S. or around the world. If we think about the Yankees cases as an example — if these are low-level infections unlikely to produce disease or even much transmission, do they represent an additional risk for viral mutation? Can the virus continue to evolve through these low-level infections in vaccinated people?
It’s a good question. There’s a big debate about it actually. If you have no immunity at all, and the virus is able to replicate in huge numbers very quickly, as it does in any ordinary first infection, that is potentially a lower-risk situation, because even though the virus grew to such great numbers, it didn’t bump into any antibodies along the way it had to figure out how to evade.
Which means there’s no motivation for it to evolve, right?
Right. And so if you already have an antibody response — because you’ve been vaccinated or you’ve been previously infected — in that case maybe the virus is only able to grow to a million titers instead of a billion … Well, those million viral particles per ml are each bumping into your already-existing antibodies, so there is actually something for them to try to learn how to evade. That’s when, theoretically, you would see the most likely scenario for immune evasion and mutation that would improve the virus’s fitness against immunity — specifically in those people who have already been vaccinated or infected and who are getting re-exposed and reinfected.
That’s the theoretical piece. But you have to layer on top of it community transmission. And if through vaccination you can drop everyone’s viral loads and transmissibility by 90 percent, then overall you should expect at a community level to have just many fewer infections. And so that should hopefully balance out that potential increase of evolutionary capacity. In other words, they’re really competing forces — do you want no immunity, and to just keep having viruses transmit unabated, or do you want to have immunity, giving the virus something to learn from, but overall have it happen in many, many fewer people? We don’t really know which exact way it balances out.
That sounds potentially scarier than I was expecting.
Well …
No?
If people aren’t getting sick and people aren’t really transmitting from these post-vaccination PCR positive infections, regardless of whether it’s a variant, then there is a chance that we could celebrate such reinfections.
What do you mean?
As I was saying earlier, we have to be careful in how we interpret the PCR and how scientists, physicians and the public equate test positivity with disease. To equate the two is a mistake. Our immunity needs to train. We have an immune system that is literally built on repeated exposures in order to elicit long-lasting immunity. This is pretty darn constant. When I evaluate the immunological profiles of young children from birth, I see that most kids see seasonal coronaviruses or adenoviruses or rhinoviruses many times in their first years of life. If not for multiple repeated exposures in time, it is very likely that by the time an individual reached 30, immunity from a single infection when they were a baby would be largely diminished. And then, if the 30-year-old got exposed, they might get sick. On the other hand, if they were exposed repeatedly after the first infection, then each exposure would potentially allow the virus to grow a bit and it would solidify immune memory against that pathogen, in the same way that studying for a test solidifies memory.
Going back to the Yankees — if no one is getting sick and spread is controlled since the first event, then in some ways a re-exposure may not be a bad thing but rather can be seen as immunological training. Is it ideal? No, of course we want this damn virus to be eliminated. But, frankly, if I am entirely vaccinated and those around me are vaccinated and I was asked in a few months “Do you want to be asymptomatically exposed” there is a world where I might say “Yes — getting exposed while otherwise protected can boost the depth and breadth of my immune response for years to come and might even improve my ability to deal with variants.”
To be clear — I do NOT advocate for this, but I do want to make clear that as long as this virus isn’t causing a vaccinated person illness, then an exposure that can be detectable on a PCR (which implies it replicated) is not necessarily a bad thing but can be seen as a free, robust booster.
I recognize the notion is a bit controversial, but biologically, it is simply how our immune systems work. Repeat exposure is important — it’s the reason we design vaccines with booster shots.
So these low-grade infections would be like free boosters.
If they’re low-grade enough to not produce sickness, yes.
So there’s little downside to getting infected after you’ve been vaccinated?
Well, I wouldn’t say that. First and foremost, if you can transmit despite not getting sick, then such exposures pose a public health risk to those who are not yet protected, even if they are serving to boost your own immunity. This is particularly important as it pertains to being around the elderly – even those who have been vaccinated. Elderly aren’t good at holding on to their immune memories and so we have to be very careful in our assumptions that vaccinated people are protected. I suspect that, come late fall and winter we will see renewed cases and these will spill into the ederly vulnerable population whose immunity will have waned sufficiently by then… a year since vaccination… to allow them to become ill if reinfected from someone who is exposed, infected but because of vaccination, not sick and not worrying about if they are exposed.
Also, immunity is rarely 100% and so if you are getting exposed post-vaccination, even if you aren’t elderly, there will still be a chance that you’ll get sick. Though this doesn’t seem to be very common and when people do get sick it doesn’t appear to be particularly severe. How long that kind of protection lasts though… time will tell.
This interview has been edited and condensed for clarity.



























